
So the first week went by in a bit of a haze. At first I’ll admit I couldn’t stop crying for about 3 days. I kept getting flashbacks to the position my knee was in during the accident & to the popping noise. The shock of new found immobility, impact on family, work, sport saw me have some dark days. I felt like my brain had turned to total mush as I couldn’t even remember what painkillers I’d taken & when.
This at the end of the day is a “just” a knee injury. But, whoever you are & whatever your injury is it will still have a impact on your quality of life & mental health in the short term. This is individual to everyone & can’t be overlooked in the patient journey.

Obviously sleeping was pretty uncomfortable & difficult to get with new found lack of activity or exercise I didn’t feel that tired. That with my new found Netflix obsession hasn’t been helping my sleep hygiene!
It’s actually been quite useful not being at home & tempted to do things. I’ve listened to my own advice of RICE. Rest, ice, compression & elevation. What do you know ..,it’s paid off! With any Physiotherapy rehab it can be difficult but have a goal in mind & hold up your end of the bargain. Half hearted attempts are unlikely to get the job done.
I’ve kept my leg elevated above the level of my heart pretty much for 50mins of every hour, iced every other hour and done simple range of movement and quads exercises atleast 5 times a day. Consequently, when I saw the orthopaedic surgeon here in Steamboat Springs, Colorado, on Monday he said the swelling had gone down enough & range of movement improved enough that he would have been willing to operate that day. However, US healthcare costs being what they are I’ve opted to return home, rehab 4-6weeks prior to surgery.
In an ideal world I would have accessed a “game ready” or similar ice compression machine which are unavailable to rent here. They are really useful to aid pain and swelling management in acute injuries. Also a muscle stimulator to facilitate thigh muscle (quadriceps) contraction would also be useful.
The other thing I have been doing is regular anti-inflammatories (ibuprofen) & paracetamol. I would very rarely take either & one thing I commonly hear patients say is that they don’t like taking painkillers or “masking” the pain. However, regular analgesia & anti-inflammatories (assuming no contraindications) in the short term may enable you to reduce excessive swelling, get the exercises done, improve range and return to function quicker which is a big bonus! Also if I’m more comfortable I’m more likely to get some sleep which we know is incredibly important in recovery.

I’ve achieved 0 degree extension (with caution) to 100 degrees flexion currently. I am walking but always with my brace on, even to the bathroom as the knee feels very unstable. It is now fixed to 0-90 degrees flexion on advice of the orthopaedic surgeon. I’m also wearing compression stockings & taking a baby aspirin to prevent deep vein thrombosis (DVT) due to immobility.
So the MRI report came through 1 day after injury. Remember how I said that those ligament tests weren’t always the most specific (testing what you think they’re testing & avoiding false positives) or sensitive (unlikely to overlook a structure your testing or avoiding false negatives)? Well it turns out there was also damage to the Lateral collateral ligaments (LCL) on the outside of the knee, which seemed fine on initial testing. However, it is often difficult to tell in an acute knee injury hence the need for further investigation. Also with an acute injury it can be difficult to assess deeper structures such as meniscus of the knee (cartilage) due to reduced movement and pain inhibition. The LCL injury was somewhat of a surprise given the mechanism of injury (how the injury occurred). Essentially I put a lot of strain on the inside of my knee. But having thought about it there was also a lot of rotation of the shin bone which may account for the damage to the LCL & posterior lateral corner.
So the MRI report makes quite a list…..:
-Total rupture Anterior Cruciate Ligament (knee joint ligament that prevents shin bone moving forwards on the thigh bone)
-Sprain Medial Collateral Ligament
(Ligament on the inside of the knee, usually braced)
-Tear posterior horn Medial Meniscus
(The back of the c -shaped ring of cartilage in the knee which provides cushioning & improves congruency of the knee. Injury is common alongside ACL injuries)
-Partial tear Lateral Collateral Ligament (ligament on outside of knee)
-Evidence of posterior lateral corner injury including the arcuate ligament
(Basically a complex interaction of both static & dynamic stabilisers on the outside of the knee, usually treated with brace in extension but this was not the consultants advice in my case)
-Medial & lateral tibial plateau bone contusions (bone bruises which are to be expected in this type of ligament injury)
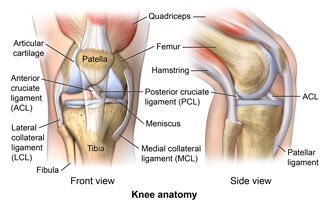
Now I could just try to rehab this knee & see how I fair & what function I can achieve. However, I’ve damaged 3 of the 4 main ligaments of the knee as well as meniscus & the posterior later corner. Ligaments connect bone to bone & provide stability to the knee. The cartilage provides cushioning & improves the congruency of the knee. Given the multi-ligament damage & my goals of returning to running & skiing my personal choice is to opt for surgery.
In order not to compromise possible ACL reconstruction it is going to be important to ensure that the other ligaments including the posterior lateral corner are either well healed or managed surgically as well if there is more damage than expected.
So there we go! More than was bargained for but not insurmountable with the right surgery & truck load of rehabilitation. For now the family are enjoying their last day of champagne powder before we start the journey home.
Tips for acute knee injuries:
-Rest – limit you’re activity & be guided by your pain & swelling.
-Ice – 20mins every other hour with bag of peas ,ice packs, cool packs wrapped in a damp cloth or game ready or similar ice compression machine. Ensure skin is going pink & not white, so as not to give yourself an ice burn.
-Compression – ACE wrap at all times except when doing exercises. Also apply compression when icing.
-Elevate- try to keep the knee above the level of your heart for 50mins in every hour.
– Take regularly NSAIDs and painkillers as directed by your doctor to enable adherence to exercises and improved mobility.
-Get lots of sleep and try to avoid turning into a night owl.
-Do your regular exercises as prescribed by your physiotherapist!
-Eat a balanced nutritious diet. Despite the lack of activity this is not the time to be dieting. You need to fuel your body for recovery.

Helen-hallo sorry to hear about your injury
I reckon you just need to solve the ACL and MM -the rest will heal.
Get a good surgeon, preferably using the more modern techniques-even in the last few years its changes
(Google-arthrex flip cutter)-this is my choice. It replicates the normal anatomy more so than previously
Good regards
Paul Macnamara
LikeLike
Thanks Paul! Agree surgery seems the obvious option with that much going on, given level of activity I want to get back to. Are you still overseas? H x
LikeLike